
Antigen (Nasopharyngeal/Oropharyngeal Swab)
The virus or nucleic acid test (see chart above) is useful mainly during active infection, before the virus is cleared by the immune system. This test is mostly used for diagnosing active infection in individuals suspected of having COVID-19, especially people with symptoms of the illness. If a virus test is positive, it is almost certainly correct (very specific). However, the test may not always detect the virus when it is present (less sensitive). In a person with COVID-19, the test is less likely to give a positive result late in the course of infection once the virus has been cleared by the immune system, or if an inadequate sample is taken from the nose or throat. A virus test normally takes an hour or less but must be done in a specialist laboratory, which can delay the result.
For an individual with symptoms, a virus test will help them get the right care, especially if clinicians are unsure if they have COVID-19 or another disease that mimics it. Knowing an individual has the illness also means they can be instructed to self-isolate at home to protect their friends, family and other members of the public from getting infected. If they are seriously ill, they can be treated in hospital with precautions to protect healthcare workers. Rapid diagnosis of individuals using the virus test can also allow tracing and isolation of people with whom an infected person has come into contact.
Antibody Test (Whole Blood/Serum/Plasma)
The antibody test (blood test) will only detect infections after the immune system has produced antibodies that recognise the virus. This happens approximately 7–10 days after symptoms develop.[2]
There is substantial work ongoing to develop accurate antibody tests for coronavirus infection. To be useful in reporting past infection and immunity in individuals, these new tests must fulfil three criteria.
First, if some people do not produce detectable amounts of the antibody used in the test after infection,[3] or if antibody levels wane with time, the test will be insufficiently sensitive, missing too many infections (false-negative results) to be useful. Second, the test must be specific enough to give high confidence that a positive test result is correct (not a false positive). This is especially true if past infection is uncommon among those who are tested, as in the general population. Infection is likely to be more common among people at higher risk, such as health workers. Third, before an antibody test can be used to indicate that someone is immune to further infection, the level of protection must be demonstrated in experimental trials. While there is a clear link between the presence of the antibody and protective immunity for many common viral infections, this has not yet been confirmed for the new coronavirus. It is possible that people are temporarily protected against reinfection but the protection wanes with time, or that protection operates against current but not future strains of the new coronavirus.
For all these reasons, antibody tests are likely to be most useful for studying past infection in whole populations to assess the scale and spread of the COVID-19 outbreak
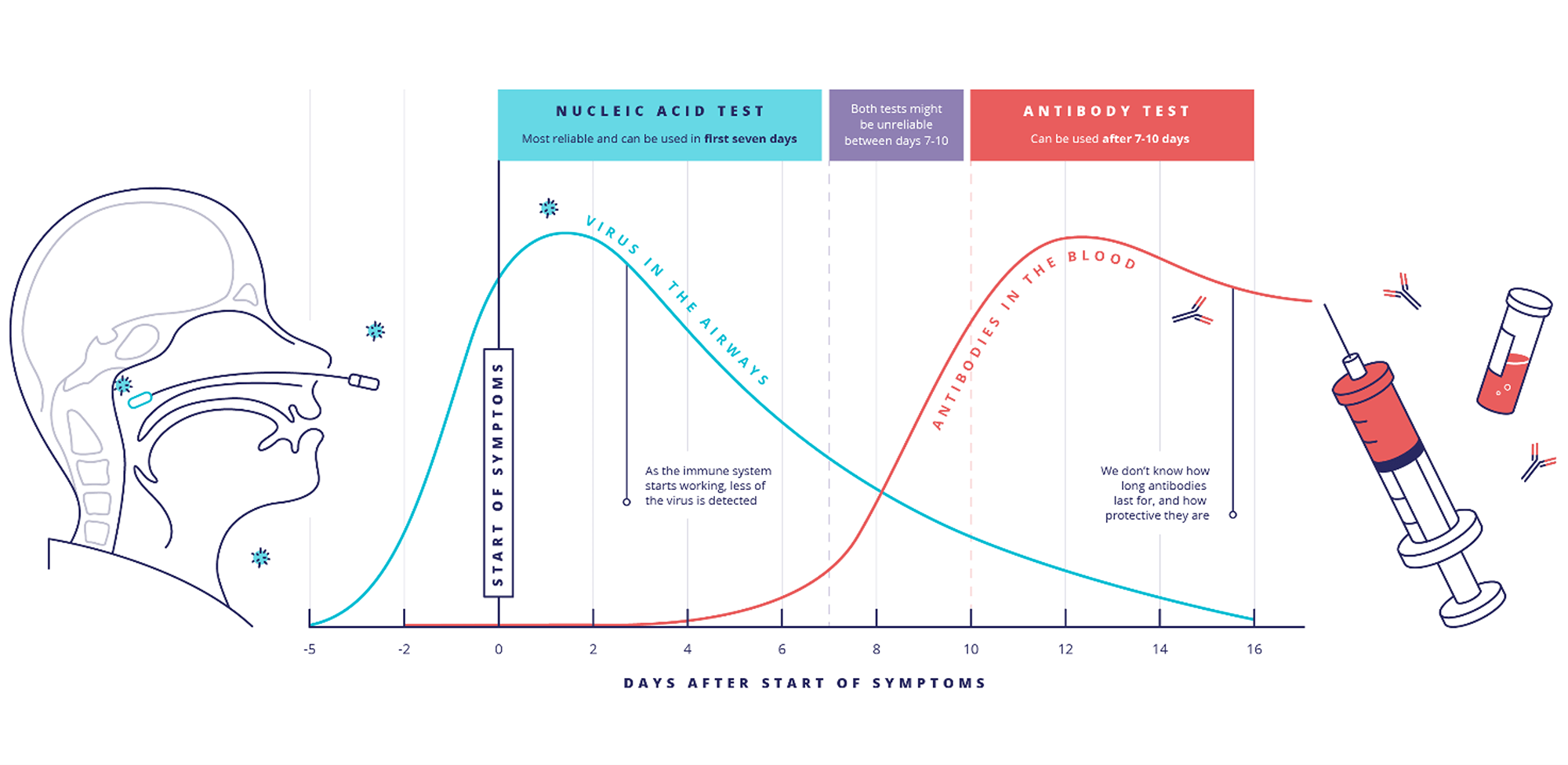
Testing for COVID-19. Virus testing is used mainly for diagnosis of active infection. Antibody testing is used mainly in surveys to assess the extent of COVID-19 spread in a population.

Source: https://coronavirusexplained.ukri.org/en/article/vdt0006/